Before moving on check out the PEMSHORT/CUTS video on using the Panoptic Ophthalmoscope
www.vimeo.com/pemcincinnati/panoptic
Corneal abrasions
Can only be diagnosed reliably with fluorescin under a Wood's lamp (black light). It may be advantageous to use tetracaine during the instillation of fluorescin. Otherwise saline will suffice. Fluorescin is safe to instill in any eye - even in an open globe. Please let your patients know that the tetracaine will burn during instillation. The treatment generally consists of topical antibiotics - I'll ask the parent which type (erythromycin ointment or polytrim drops) they would prefer. Generally corneal abrasions will heal well in less than a week, antibiotics can help reduce the already low risk of infection.
Foreign bodies
Everting the top eyelid can allow you to visualize a foreign body which is usually behind the upper lid. Removal of material adherent to the inside of the upper lid can be done with a cotton swab, flush with saline, or needle nose forceps. Removing a foreign body off of the surface of the eye can be done (delicately) with an 18 Guage needle to 'flick' it off of the eye. Topical antibiotics are always appropriate.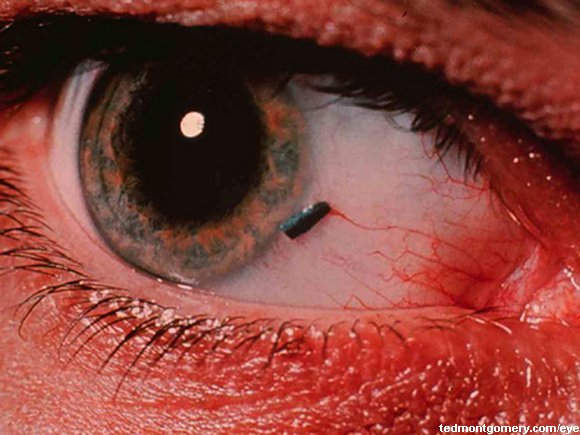
Abnormally shaped pupil
A pupil that is not a circle is bad. This generally indicates that the ciliary muscles of the iris have been disrupted/compromised. This can be due to direct trauma or an open blow.Traumatic iritis
Look for the patient with decreased visual acuity and extreme light sensitivity.
Hyphema
Blood in the anterior chamber will create a meniscus like effect. These occur usually due to ocular trauma. The biggest risk is of acute angle closure glaucoma. The treatment is bed rest - for patients with a a hyphema >25-50% of the anterior chamber admission might be warranted. Rebleeding can occur - and the risk extends into and in some cases beyond the second or third day.
The open globe
Generally fluorescin adheres to epithelium. Fluorescin that 'flows' is generally floating on the aqueous material. This is AKA Seidel's sign. The classic 'tear drop' shaped pupil is an important finding to recognize.
Uveitis and hypopyon
White fluid in the anterior chamber - similar to a hyphema - is a hypopyon which can be infectious or inflammatory.
General pearls
1. The visual acuity is the vital sign of the eye2. Always ask patients with eye infections whether or not they wear contacts
3. Use the panoptic ophthalmoscope for a much better view of the retina and fundus
No comments:
Post a Comment